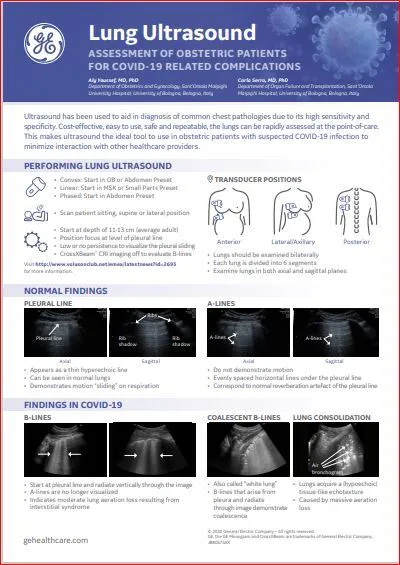
Pregnant women may be at a higher risk of developing dangerous respiratory infections than the general population, according to the American Journal of Obstetrics and Gynecology. This is a concern regarding COVID-19. Currently, the gold standard used for diagnosing COVID-19 is a real-time analysis of respiratory tract specimens, along with a chest CT scan. Since evidence of the disease does not always show up until later in the infection, tests are often repeated. However, this is not ideal due to radiation exposure from the CT.
Fortunately, there is another option. Lung ultrasounds have been found to be as effective as the chest CT at detecting lung consolidation and other signs of viral pneumonia, as reported by Intensive Care Medicine. Using ultrasound assessment in cases of suspected COVID-19 can help limit the need to transport a seriously ill or contagious patient and allows physicians to image patients who would not otherwise be able to tolerate a CT scan, including pregnant women.
Because ultrasound examination is often most familiar to obstetricians and gynecologists, these clinicians are in an ideal situation to provide lung ultrasounds for existing obstetric patients. OB/GYNs who do not currently use ultrasound may consider adding it to their clinical practice.
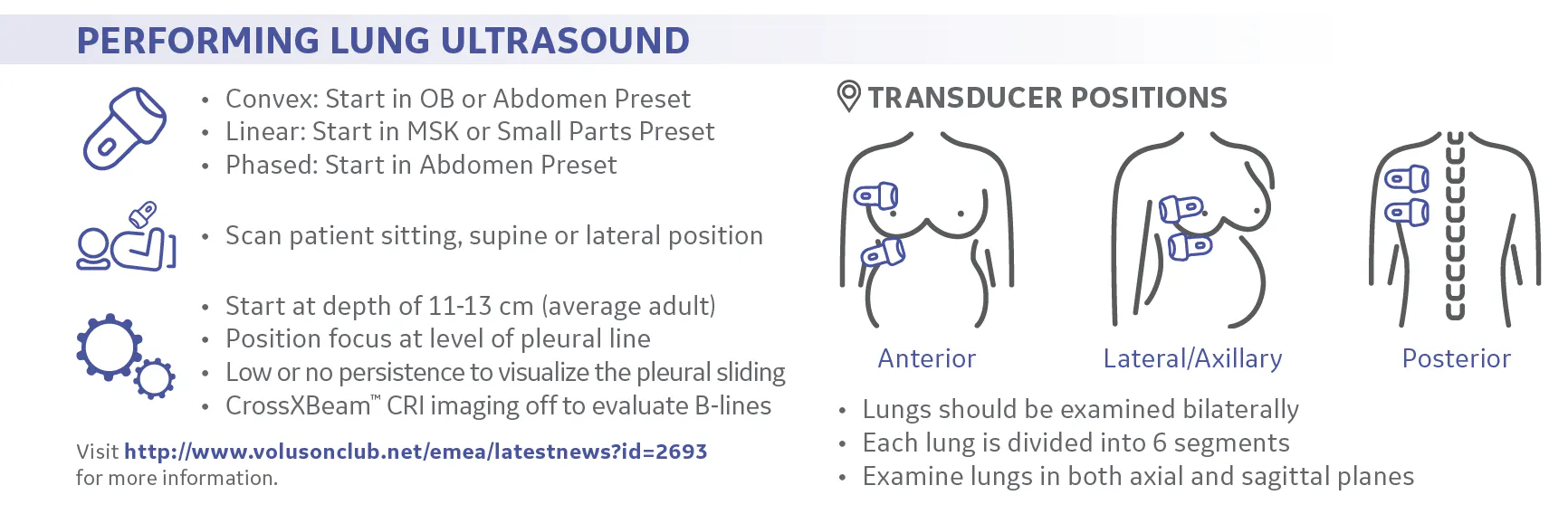
Setting Up for a Lung Ultrasound
Each hemithorax of the lungs is divided by the anterior and posterior axillary lines into six parts: two posterior, two anterior and two lateral regions. Each region is assessed in both longitudinal (sagittal) and transverse (axial) planes. In order to assess all regions of the lungs, patients must be assessed in multiple positions: sitting erect, supine, prone and left and right lateral decubitus. Either a linear or a convex ultrasound transducer can be used, depending on the patient's body habitus.
The recommended locations for performing lung ultrasounds are either at the patient's bedside, for a person with suspected COVID-19 symptoms, or in the provider's practice, for a routine obstetric ultrasound exam intended as preventative care to rule out any possibility of the disease. Handheld or cordless ultrasound transducers may be preferred, as they are easier to sterilize.
In cases of suspected COVID-19 infection, it is best to follow all recommended safety precautions. For instance, the transducer should be covered with a protective sheath and cleaned according to the manufacturer's recommendations. The ultrasound machine should be completely disinfected after use, and the clinician or technologist performing the ultrasound should wear gloves, a full gown, a mask and a face shield.
Normal Lung Appearance
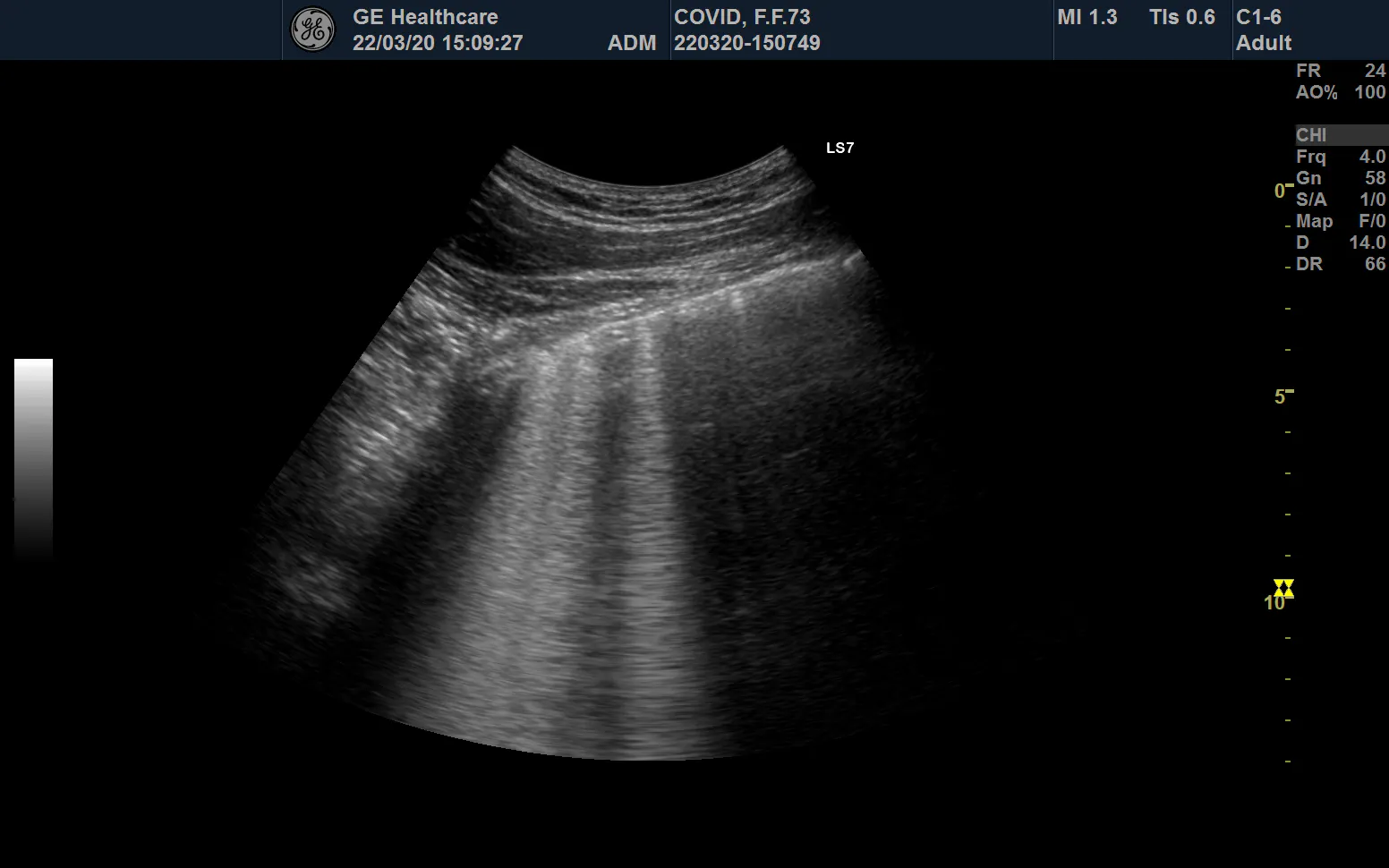
In a normal lung, the aerated pulmonary parenchyma causes acoustic mismatch and reflection of the ultrasound beam, which prevents direct imaging of the lung parenchyma. However, ultrasound is able to clearly visualize subcutaneous tissues and lung pleura. The pleura is seen as a strongly echogenic horizontal line between the ribs. Parallel and posterior to the pleura are the "A-lines," echogenic artifacts caused by reverberation that are a normal finding.
Positioning the transducer in the longitudinal plane of the lung area allows for visualization of the bright echogenic pleural line, which slides easily in a superior-inferior direction with the patient's respiration. A-lines are visible, posterior to the pleura, as regularly spaced horizontal lines. Ribs will show at regular intervals and give off strong, sharp posterior shadowing.
Rotate the transducer into the transverse plane and the pleural line, and A-lines will appear again, but without the rib shadowing. For a normal, healthy lung, a cine clip taken in both of these planes will demonstrate the thin, regular pleural line with smooth pleural motion.
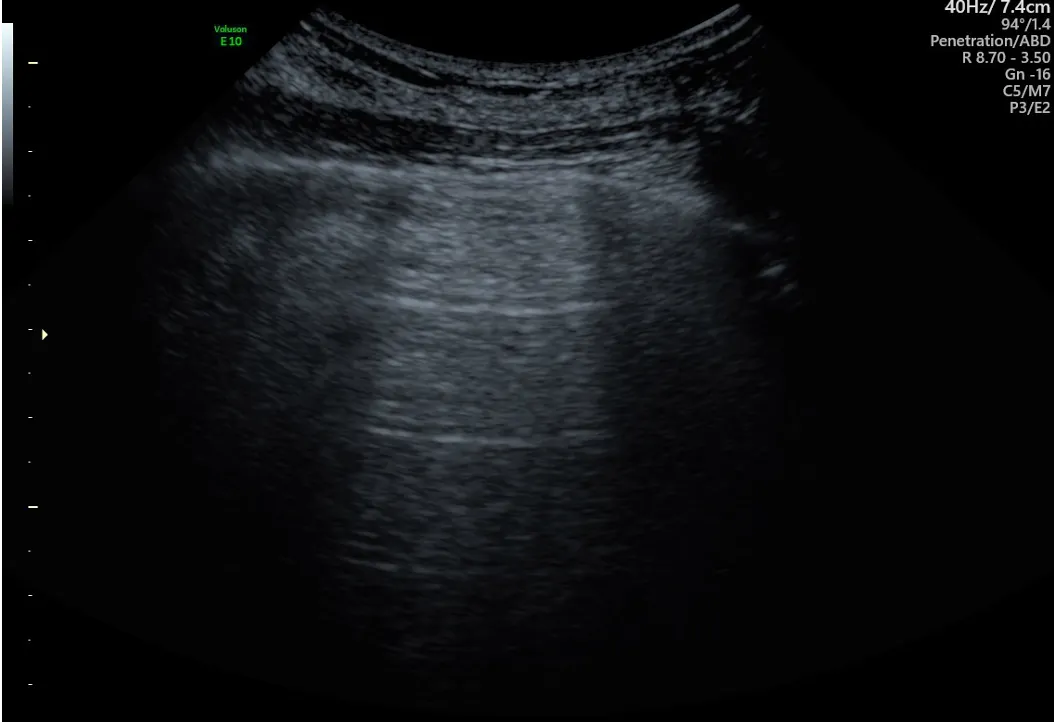
Transverse view of normal lung. Image courtesy of Dr. Aly Youssef
Abnormal Lung Appearance
An abnormal lung affected by pneumonia or other respiratory issues can partly lose aeration, become consolidated, be inflamed or contain edema or a pleural effusion. An abnormal lung has a distinct ultrasound appearance in COVID-19 patients, according to guidelines published by the International Society for Ultrasound in Obstetrics and Gynaecology (ISUOG).
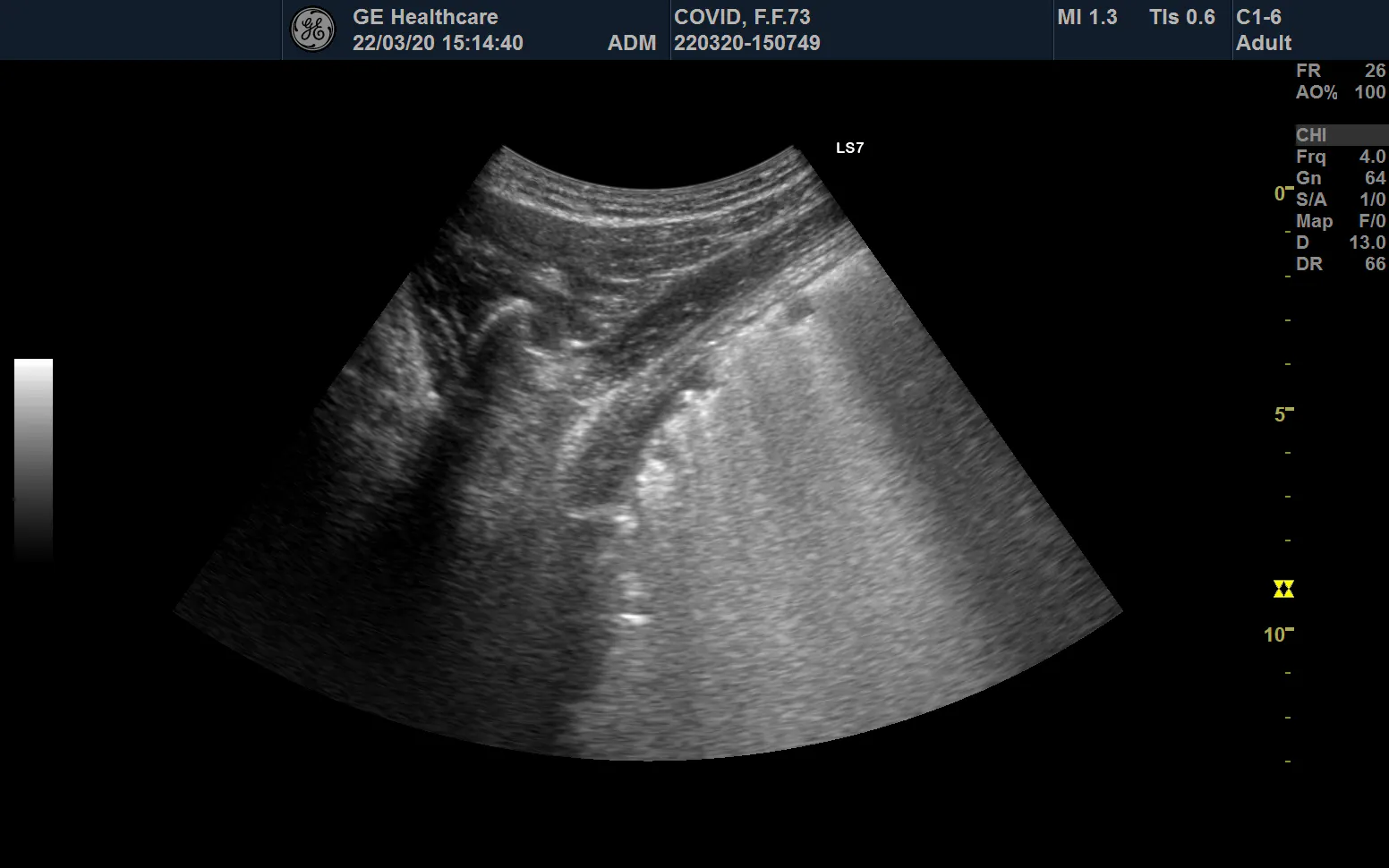
B-lines are vertical artifacts of different shapes and sizes that extend vertically from the pleural line. They result from abnormal gas-tissue interface and are seen when the lung begins to lose normal aeration. A thickened, irregular or blurred pleural line with posterior enhancement (known as ultrasonic "white lung") indicates inflammatory lung disease, seen in early-stage COVID-19.
Ultrasound image showing B-lines. Image courtesy of Dr. Aly Youssef
2D ultrasound demonstrating "white lung". Image courtesy of Dr. Aly Youssef
An irregular hypoechoic area seen at or around the pleural line is evidence of massive aeration loss resulting in a partly or completely collapsed lung. When the lung loses air, the organ appears solid and can be more completely evaluated through ultrasound. Posterior anechoic collections demonstrate the presence of a pleural effusion. These effusions can be either simple or complex fluid and are so far observed to be rare in COVID-19 infections.
Adding Lung Assessments to OB/GYN Ultrasound Exams
Although lung ultrasounds are limited to assessing the peripheral pleural layer, they are still able to recognize specific and significant signs of pneumonia and infection that are characteristic of COVID-19. Obstetrical ultrasound examinations, already safe, readily available and radiation-free, can be extended to include lung ultrasounds to provide proactive care for pregnant women with suspected COVID-19.