
Join Dr. Liona Poon for an expert presentation with GE HealthCare on the Tips and Tricks of Intrapartum Transperineal Ultrasound. This talk focuses on the benefits of ultrasound in labor and delivery, for both the patient and physician. Dr. Poon is a chairperson and clinical professor at the department of obstetrics and gynaecology at the Chinese University of Hong Kong and one of the authors of the Feasibility, Reliability, and Agreement of Transperineal Ultrasound Measurement: Results from a Longitudinal Cohort Study.
The Role of Ultrasound in First-Stage Labor
Dr. Poon demonstrates how transperineal ultrasound can be a helpful tool to complement the clinical examination in labor management. The benefits of ultrasound assessment during labor (when compared to digital vaginal exams) include a reduced infection risk and improvement in patient comfort, the removal of guesswork due to clear and objective documentation of labor through sonographic images and measurements, a less invasive assessment and overall greater confidence in delegation to junior clinicians, allowing for physicians to manage more than one delivery at a time.
The following obstetrics ultrasound images and measurements can then be taken to assess position of fetal head and cervix dilation. To monitor and predict the progress of labor these measurements are taken multiple times, at repeated intervals, and change in the measurements is documented. This provides a concise reference point to determine the likelihood of vaginal delivery, removing the need for vaginal exams and guesswork.
Parasagittal Angle of Progression (psAOP) Helps Identify the Fetal Head Station
In the sagittal plane, sweep through to line up the two bony landmarks of the maternal pubic symphysis and the fetal skull. Once they are lined up together in sagittal, freeze an image.
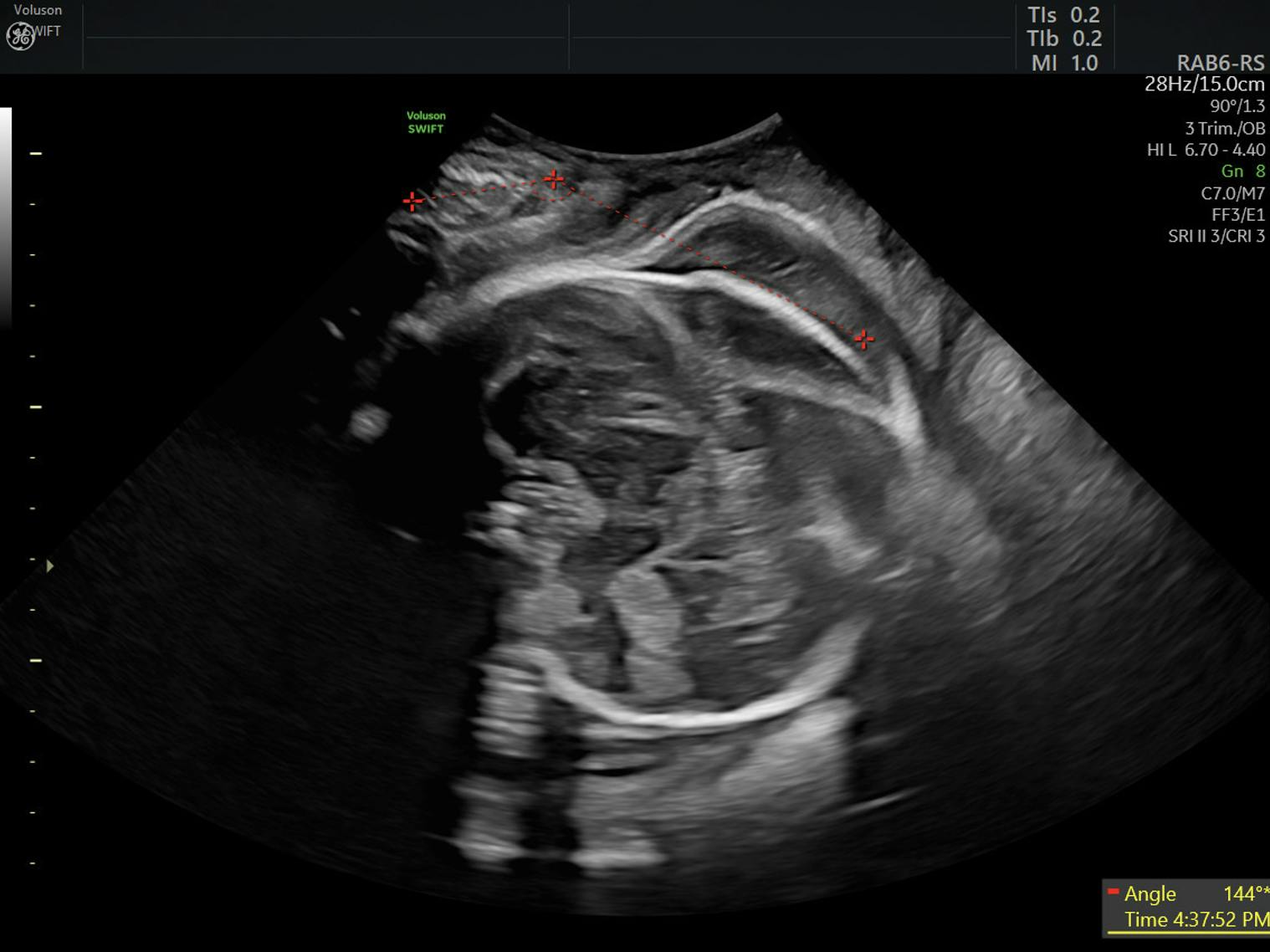
Activate the angle ruler function and place the first caliper in a line along the length of the pubic symphysis from the most superior to most inferior edge, so that it divides the pubic symphysis into two symmetrical portions. Then place the next caliper in a tangential line across the foremost edge of the fetal skull. An angle will be generated by the caliper package and printed on the screen. Save this image.
Any angle identified beyond 120 degrees is very reassuring that labor is proceeding well and that a successful vaginal delivery is likely for that patient. And an angle of near to 180 degrees tells us that vaginal delivery is immediately imminent in that patient. A series of comparative psAOP images can also be taken over time to determine if labor is progressing normally.
Head-Perineum Distance (HPD) Helps Identify Fetal Head Station
For this measurement, rotate the transducer 90 degrees counterclockwise into the transverse plane and use firm pressure on the perineum, angling superiorly until the fetal skull can be clearly visualized. Freeze an image where the fetal skull is clearly seen and use the caliper package to measure the shortest distance between the fetal head and the perineum (the most inferior/superficial aspect of the image). A series of comparative HPD images, taken over time, are often required to determine if progression of labor is occurring normally.
Sonographic Cervical Dilatation (SCD)
In the transverse plane, identify the maternal cervix, located just inferior/posterior to the fetal head. To locate the best view you can, begin in the sagittal plane, place the cervix in the center of the image and rotate the transducer 90 degrees counterclockwise into the transverse plane, while keeping the cervix in the image. Once identified, freeze a transverse image of the cervix, with the central hypoechoic cervical lumen clearly demonstrated. Then an anterior-posterior (AP) measurement is taken by placing the calipers vertically from the anterior edge to the posterior edge of the endocervical lumen. This will provide a measurement of the degree of dilation of the cervix.
The Degree of Caput Present Around the Fetal Skull
Diagnosis of caput during labor is often variable, depending on who conducts the assessment. However, transperineal obstetric ultrasound improves caput determination by providing a more objective assessment method with documentation.
Caput assessment with transperineal ultrasound allows for imaging and assessment in both the transverse and sagittal planes, as well as measurement of the area of caput. To measure the caput, identify a sagittal plane view that includes both the fetal skull and cervix. Freeze this image and place one caliper on the most inferior edge of the fetal skull and the second caliper on the outer edge of the hypoechoic caput demonstrated in the image. Caput can change over time, so a series of comparative images with measurements can be useful.
The Degree of Molding Present Around the Fetal Skull
Transperineal ultrasound can be used to visualize the degree of molding present in the fetal skull, or the overlapping of sutures of the skull that occurs during labor. More information on how to use ultrasound to assess molding will be explored in future research.
Practical Considerations for Patient and Fetal Care
By integrating intrapartum ultrasound into the clinical examination during labor, the physician can acquire confirmed facts about the fetus and maternal cervix, which allows for more precise information about the progression of labor. Intrapartum ultrasound can also confidently demonstrate the following important factors in labor: fetal heart presence and rate, fetal lie (whether it be longitudinal, oblique or transverse), fetal presentation (cephalic or breech), fetal position (OA, OT or OP), as well as fetal station, cervical dilatation, caput and molding.
Some of the challenges to intrapartum transperineal ultrasound include the following:
If the patient's bladder is full it displaces the fetal skull deeper in the image, which prevents clear visualization of the skull and accurate measurements. So the patient bladder must be completely empty to take accurate measurements. When the fetal head is located very high (superior) in the pelvis, it results in reduced image quality, poor visualization and less accurate measurements. Some of these measurements cannot be done when the fetal skull is too high. When performing the transperineal ultrasound, firm pressure with the transducer may be required for clear images, however care must be taken that pressure is applied slowly and gently to not cause further pain to the patient. Also avoid any pressure on the maternal clitoris as this results in pain and discomfort.
The Benefits of Ultrasound During Labor
The intrapartum ultrasound assessment and measurements of psAOP, HPD and SCD have been found to correlate well with traditional vaginal examinations and are both feasible and reproducible. When multiple measurements are taken at repeated intervals, the use of transperineal ultrasound is able to successfully monitor and predict the progress of labor.
Ultrasound can also provide physical evidence of intrapartum assessment, which removes the guesswork from these exams, providing patients with greater confidence in their clinician. It can even allow for the delegation of labor supervision to more junior colleagues, allowing the physician to oversee multiple labor and delivery patients, if needed. Other benefits of ultrasound assessment include improving patient comfort level through the use of less invasive ultrasound, reducing risk of infection, and providing clear documentation and record of care for the labor and delivery patient.
Hear from Prof. Poon about the feasibility of integrating ultrasound
parameters into the partogram.
Hear from Prof Poon about the possibilities to teach novice users labour
ultrasound.