
Even though it occurs relatively rarely, pediatric ovarian torsion is a serious condition requiring prompt diagnosis and immediate treatment. Left unmanaged, ovarian torsion may result in impairment or complete loss of fertility. The affected ovary may be lost without surgical intervention, but ensuring an accurate diagnosis presents a unique challenge to gynecologists.
According to a study published in RadioGraphics, 15 percent of all ovarian torsions occur in pediatric patients. In most cases, the condition develops during early adolescence and in the immediate postmenarchal years.
Diagnosing this condition in young children can be especially difficult, as they cannot always communicate their symptoms as clearly as an adult or teen patient can. Luckily, first-line imaging tools such as ultrasound offer a fast and effective method for visualizing ovarian torsion regardless of the patient's age.
Signs and Symptoms of Pediatric Ovarian Torsion
Because of its nonspecific symptoms, pediatric ovarian torsion may initially be mistaken for other emergency conditions affecting the abdominal region, such as appendicitis. The American Pediatric Surgical Association notes that clinicians considering a diagnosis of ovarian torsion should evaluate for three key symptoms:
- Pain in the lower abdomen.
- Pyuria.
- Nausea and vomiting.
Abdominal pain is generally categorized as sharp. Pain may occur suddenly, and become constant as the condition advances. In some cases, pediatric ovarian torsion may also result in an elevated body temperature or heart rate.
Ultrasound for Diagnosing Ovarian Torsion in Children
Ultrasound is the diagnostic method of choice for evaluating pediatric patients for ovarian torsion. Transabdominal ultrasound is recommended, as transvaginal examination may cause significant distress, especially if patients are not yet sexually active.
According to the Canadian Journal of Surgery, the most consistent finding on ultrasound is an adnexal mass or an echogenic mass where the ipsilateral ovary cannot be visualized. Additionally, clinicians should expect to see unilateral ovarian enlargement.
Torsed ovaries may appear unusual on ultrasound depending on the degree of stromal edema, internal hemorrhage, infarction and necrosis that has already occurred. If color Doppler is available, ovarian torsion can be easily spotted by the characteristic "whirlpool" sign.
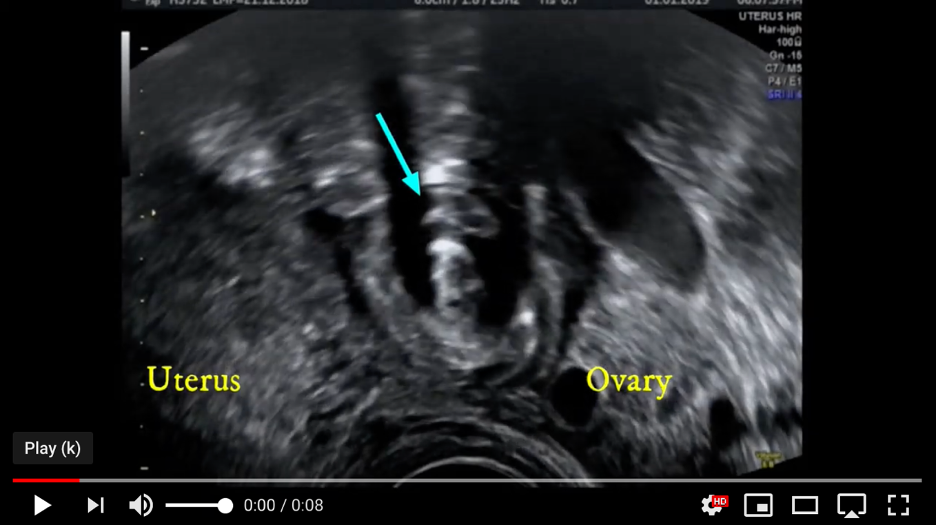
Ovarian torsion whirlpool sign on ultrasound
In many cases, ultrasound also shows ovarian follicles appearing at the periphery of the ovary, if they are visible at all. This contrasts with the normal ovarian ultrasonic appearance, in which follicles are randomly distributed through the parenchyma. Other characteristic ultrasound findings may include:
- Adnexal cysts.
- Atypical position of the ovary within the pelvis.
- Free fluid in the pelvis.
Preserving Fertility in Pediatric Patients
Timely surgical intervention is necessary to preserve the fertility of pediatric patients with ovarian torsion. The American College of Obstetricians and Gynecologists (ACOG) state that surgeons should adhere to laparoscopy using minimally-invasive methods as the treatment standard. In order to preserve fertility, surgeons should not remove torsed ovaries unless it is absolutely necessary.
This is particularly important when faced with a suspected necrotic ovary. Many providers suspect necrosis when the ovary appears black or blue. However, the appearance of the ovary during initial surgery is not a reliable indicator of its viability. In many cases, surgery restores ovarian function, and ovaries may appear near-normal during a second-look laparoscopy as little as 36 hours after detorsion.
Saving the ovary typically preserves fertility in pediatric patients, but regular followup care is essential. At minimum, doctors should obtain ultrasound images at least once post-operatively. However, if ovarian cysts or masses are noted during a followup exam, regular and frequent monitoring of the patient is recommended.

