Placenta accreta spectrum is an umbrella term that encompasses three abnormal placenta accreta types in pregnancy, each with a variable depth of placental invasion. Placenta accreta spectrum should be distinguished from placenta previa, which is the state of a placenta overlying the internal cervical os. In some cases, placenta previa and placenta accreta spectrum can coexist.
A placenta previa state with a history of cesarean section should be recognized as a red flag for placenta accreta spectrum, and a more critical assessment should be facilitated by an expert sonographer or sonologist.
Diagnosing Placenta Accreta Spectrum
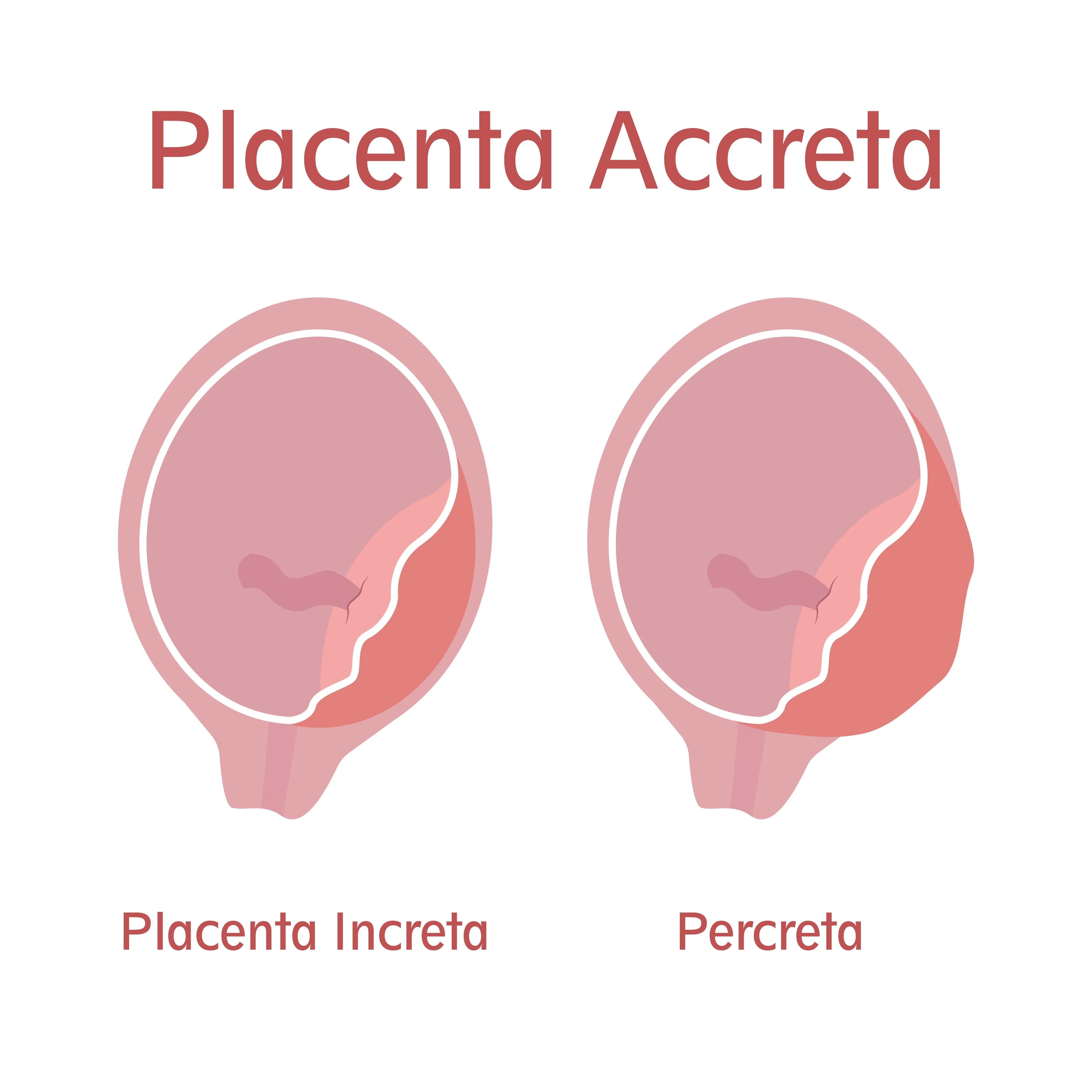
The three placenta accreta types are accreta, increta and percreta. When placental tissue implants onto the myometrium, it is called placenta accreta. When invasion extends into the myometrium, the descriptor placenta increta is used. Finally, when invasion extends through the myometrium to surrounding organs, such as the bladder, it is called placenta percreta. In short, placenta accreta spectrum can be diagnosed when there is an invasion of the placenta beyond its typical invasion depth.
Research from the Canadian Medical Association Journal notes that placenta accreta spectrum carries significant risks, including delivery by cesarean hysterectomy, massive hemorrhage, disseminated intravascular coagulopathy and, in rare situations, maternal death. Historically, this state was diagnosed incidentally at the time of delivery. Such late diagnosis may be the biggest risk factor for poor outcomes.
Today, placenta accreta spectrum can be diagnosed pre-delivery using ultrasound in most cases, allowing the patient and healthcare team to better prepare. Prenatal diagnosis of placenta accreta spectrum is fundamental for improving maternal morbidity. Early diagnosis also helps ensure treatment can occur in a center with expertise in the surgical management of this condition.
Identifying Placenta Accreta Spectrum on Ultrasound
The process of diagnosing placenta accreta spectrum should start in the first trimester of pregnancy. One of the most common markers for placenta accreta spectrum in the first trimester is a gestational sac in the lower uterine segment of a patient with a history of cesarean section, according to research from the International Journal of Gynecology and Obstetrics. Under the microscope, a cesarean scar pregnancy resembles a second-trimester placenta accrete spectrum scenario. A landmark 2013 paper from Ultrasound in Obstetrics and Gynecology posits that a cesarean scar pregnancy is a precursor to placenta accreta spectrum.
Several markers of placenta accreta spectrum can be identified using ultrasound in the second and third trimesters, as well. First, placental lacunae can be classified when irregular, hypoechoic spaces with vascular flow within the placenta are visualized. The number of lacunae (especially more than three) or their large size are two key features of placenta lacunae that may indicate a higher risk for placenta accreta spectrum.
Another feature is the abnormal uteroplacental interface. This loss of the retroplacental hypoechoic zone between the myometrium and the placenta is marked by a myometrial thickness of less than 1 mm. In most cases, this finding is seen along the posterior bladder wall.
A physician might also see an abnormal uterine contour, also known as a placental bulge. In some cases, this bulge can be so severe that placental tissue is visible extruding beyond the uterine serosa.
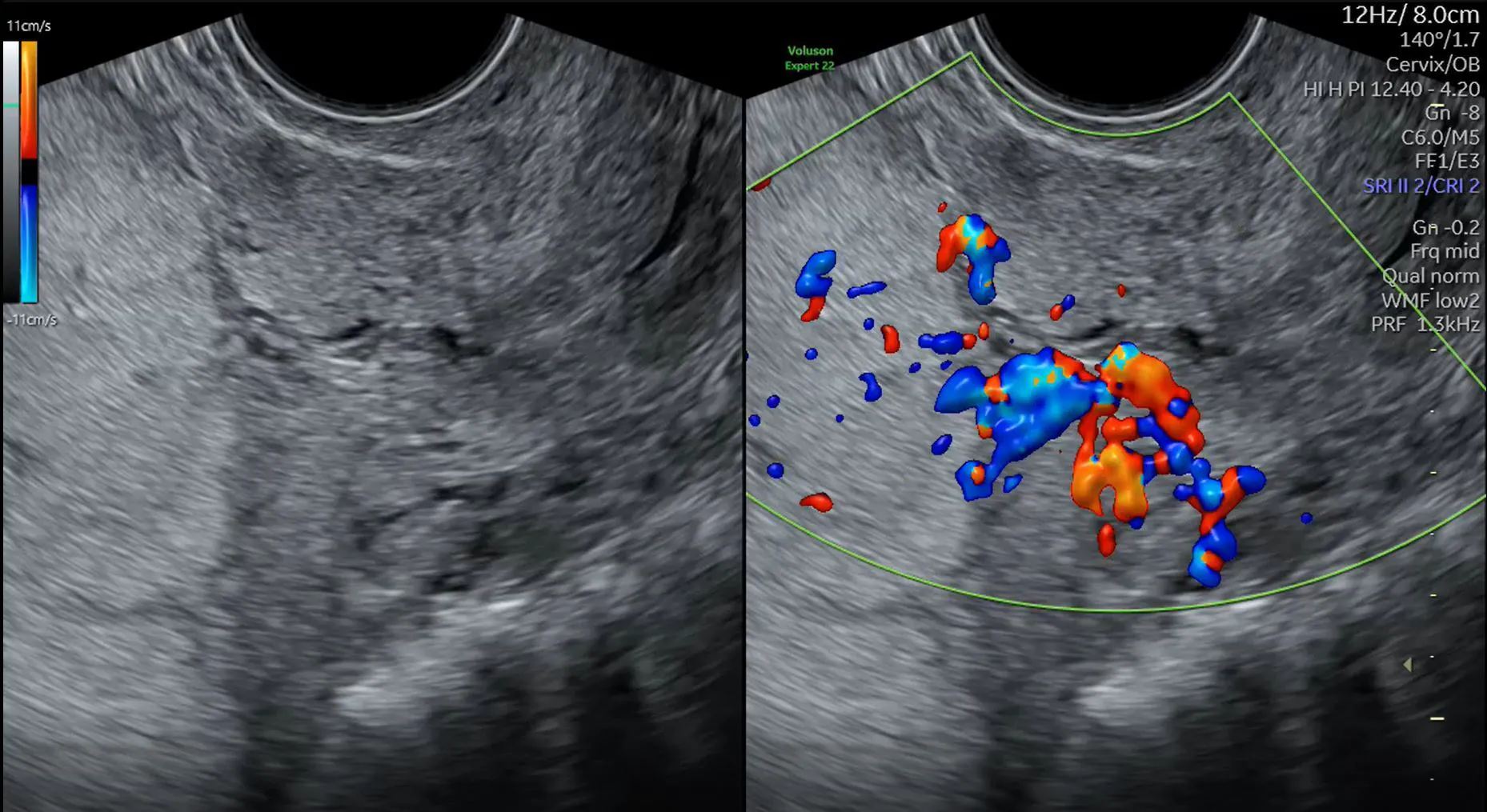
Finally, research published in the American Journal of Obstetrics and Gynecology reports that ultrasound with color Doppler can reveal bridging vessels extending from the placenta across the myometrium and beyond the uterine serosa.
Organizing the Care Team
Once placenta accreta spectrum is diagnosed, it is essential that treatment takes place in a healthcare facility that has experience managing these cases. A multidisciplinary care team should involve or include:
- Advanced gynecologic surgeons
- High-risk obstetricians
- Anaesthesiologists
- Neonatologists
- Psychology or social work services
- Blood conservation
- Interventional radiology
According to research from the Journal of Obstetrics and Gynecology Canada (JOGC), the earlier the referral, the more optimal the management. Better management reduces the need for massive transfusion and multiple surgical interventions, improving maternal outcomes.
In many cases, a cesarean hysterectomy needs to be planned in conjunction with treatment, balancing maternal and fetal outcomes. In scenarios where a patient wants to preserve their future fertility, alternative surgical options exist. However, these are associated with a protracted course of recovery and a persistent risk of hysterectomy, according to the JOGC researchers.