
Although first trimester bleeding is common — occurring in 15 to 25 percent of pregnancies, according to the American College of Obstetricians and Gynecologists (ACOG) — it understandably causes many patients to fear the worst. Even if bleeding does not end in a miscarriage, a study published in Obstetrics and Gynecology shows that more than one day of bleeding in the first trimester is linked to lower birth weight. Understanding the potential causes of bleeding in early pregnancy and knowing how to respond helps reproductive endocrinologists calm their patients' fears and support a healthy pregnancy.
Implantation Bleeding
If an embryo successfully implants, the process itself might cause the patient to experience implantation bleeding. Implantation typically occurs between one and three days after an embryo transfer, and this type of bleeding is most likely to occur shortly afterward. Patients carrying multiples may be more likely to experience implantation bleeding.
Unfortunately, implantation bleeding symptoms mimic PMS and generally happen around the time a patient might expect their period. Implantation bleeding is typically lighter in flow (more like spotting or light bleeding than full menstruation), color (light pink to dull brown in color rather than bright or dark red), and duration (a few hours to a couple of days) than the patient's normal period.
More potential symptoms include:
- Backache.
- Headache.
- Nausea.
- Breast tenderness.
- Mild cramping.
The best way to diagnose implantation bleeding is through hCG level monitoring. If the patient's symptoms match those described above and early hCG levels double every 48 to 72 hours, the bleeding was most likely as a result of implantation.
Cervical Changes
Pregnancy changes a patient's normal hormone production and increases blood flow to the cervix, which makes the cervix more prone to bleeding. Additionally, 2 to 5 percent of women develop cervical polyps, according to research published in the International Journal of Reproduction, Contraception, Obstetrics and Gynecology. Irritation, inflammation or any contact with the cervix — caused, for example, by a polyp, intercourse or a transvaginal ultrasound exam — may result in light, bright red first trimester bleeding.
A diagnosis often comes after examining the cervix during a routine pelvic exam. This type of bleeding will cease on its own and requires no physician follow-up. However, many doctors advise patients to avoid penetrative intercourse until after a strong heartbeat has been confirmed — or even until after shifting from the fertility clinic to an OB/GYN.
Subchorionic Hemorrhage
A subchorionic hemorrhage is when blood collects between the gestational sac and uterine wall. Some studies suggest that hemorrhages are the most common type of first trimester bleeding, but this theory is disputed. Research published in Obstetrics and Gynecology reports that past studies have found a prevalence of anywhere between 1.3 and 62 percent depending on the population studied.
Although not all researchers agree on the specific cause, some hemorrhages may occur when the placenta partially or fully dislodges from the uterus. Pregnancies conceived via IVF using frozen transfers and embryos with a B or C grading, in particular, may increase the chances of hemorrhages.
Symptoms may include:
- Light to very heavy bleeding, with or without clots.
- Pink, red or brown blood.
- Cramping or lower abdominal pain.
A transvaginal ultrasound is crucial for properly diagnosing and predicting the outcome of a hemorrhage. Factors that determine the prognosis include the size of the hemorrhage, the patient's age and the gestational age of the fetus.
One study published in the Journal of Ultrasound Medicine found that hemorrhages that are small relative to the gestational sac — less than 50 percent the size of the gestational sac — tend to result in a better outcome. The study also found that patients younger than 35 who were diagnosed with a hemorrhage had a 9.6 percent rate of miscarriage, compared with 19.6 percent for patients 35 and older.
The researchers found that hemorrhages diagnosed at or before seven gestational weeks had a higher miscarriage rate (19.6 percent) compared with those diagnosed after seven weeks but before or at eight weeks (14.6) and after eight weeks but before or at 11 weeks (3.6 percent).
Reproductive endocrinologists should closely follow the hemorrhage via transvaginal ultrasound and monitor its development. Ideally, it will continue to shrink or resolve altogether.
Infections and STIs
Bleeding can be unrelated to the pregnancy itself. Your patients will likely recognize the common symptoms of a urinary tract or yeast infection, such as unusual discharge or vaginal itching and burning, but they may not know that these infections — along with bladder and pelvic infections — may cause pink to red light spotting or bleeding.
A sexually transmitted infection such as chlamydia, gonorrhea or herpes may also lead to spotting. Diagnosing and addressing the cause of the infection should resolve the bleeding.
Ectopic Pregnancy
Ectopic pregnancies are relatively rare, occurring in only approximately 2 percent of all pregnancies, according to the American Pregnancy Association. However, according to research from the McGill University Department of Obstetrics and Gynecology, IVF patients may have a greater risk of a pregnancy that implants outside the uterus.
Unlike other types of first trimester bleeding, ectopic pregnancies have risk factors, rather than specific causes. These can include:
- A previous ectopic pregnancy.
- Endometriosis.
- Prior Fallopian tube, pelvic or abdominal surgery.
- Advanced maternal age.
- Pelvic inflammatory disease.
- Some sexually transmitted infections, such as chlamydia and gonorrhea.
- Smoking.
However, as many as half of ectopic pregnancies occur in women with no risk factors, ACOG reports. The symptoms that bring a patient to the OB/GYN or emergency room may include vaginal bleeding, lower back pain, rectal pain or pressure and cramping or pain in the lower abdomen, particularly on one side.
An ectopic pregnancy can cause a patient's Fallopian tube to rupture, and can even result in death if not addressed quickly. Thankfully, approximately 75 percent of tubal ectopic pregnancies can be diagnosed with transvaginal ultrasound, according to research published in Deutsches Ärzteblatt International.
If the physician cannot confirm an intrauterine pregnancy or rule out an extrauterine pregnancy, the patient's options are medication or surgery. If the pregnancy is early and the fallopian tube is not at risk of rupturing, it may be appropriate to prescribe methotrexate.
In all other cases, the patient will need surgery, the most common being laparoscopy. One option is removing the ectopic pregnancy, if it can be done without damaging the tube. However, if the tube is damaged, the tube may also be removed. If the tube has already ruptured, the patient may need a laparotomy, an emergency surgery with a larger incision.
Many reproductive endocrinologists advise patients wait at least three months before trying to conceive again. They should also advise patients about the increased risk of an ectopic pregnancy in the future.
Molar Pregnancy or Gestational Trophoblastic Disease
Although rare, a molar pregnancy happens when abnormal placental tissue grows in place of a fetus due to a genetic error during fertilization. Sometimes, the tissue is cancerous and spreads to other areas.
Symptoms may include:
- Bright red to dark brown bleeding.
- Lower abdominal pain or pressure.
- Nausea or vomiting.
- Rapid uterine enlargement.
A molar pregnancy is diagnosed with a combination of a transvaginal ultrasound and hCG blood test. A complete molar pregnancy may be easier to detect, accompanied by higher than expected hCG levels, than a partial molar pregnancy.
Physicians will remove the products of conception with a dilation and curettage (D&C), and a pathologist will examine a tissue sample. The patient may need to consult an oncologist.
Miscarriage
Many of the complications discussed above can result in a miscarriage. Miscarriages are especially common when a patient is carrying multiples. However, sometimes the cause of a miscarriage is unknown. A miscarriage can be confirmed with a combination of hCG blood levels and a transvaginal ultrasound. Depending on the patient's age and gestational age, doctors may advise expectant-mother management, medication such as methotrexate or a D&C.
Knowing that bleeding scares patients, reproductive endocrinologists should show compassion and empathy throughout the diagnosis and treatment process.
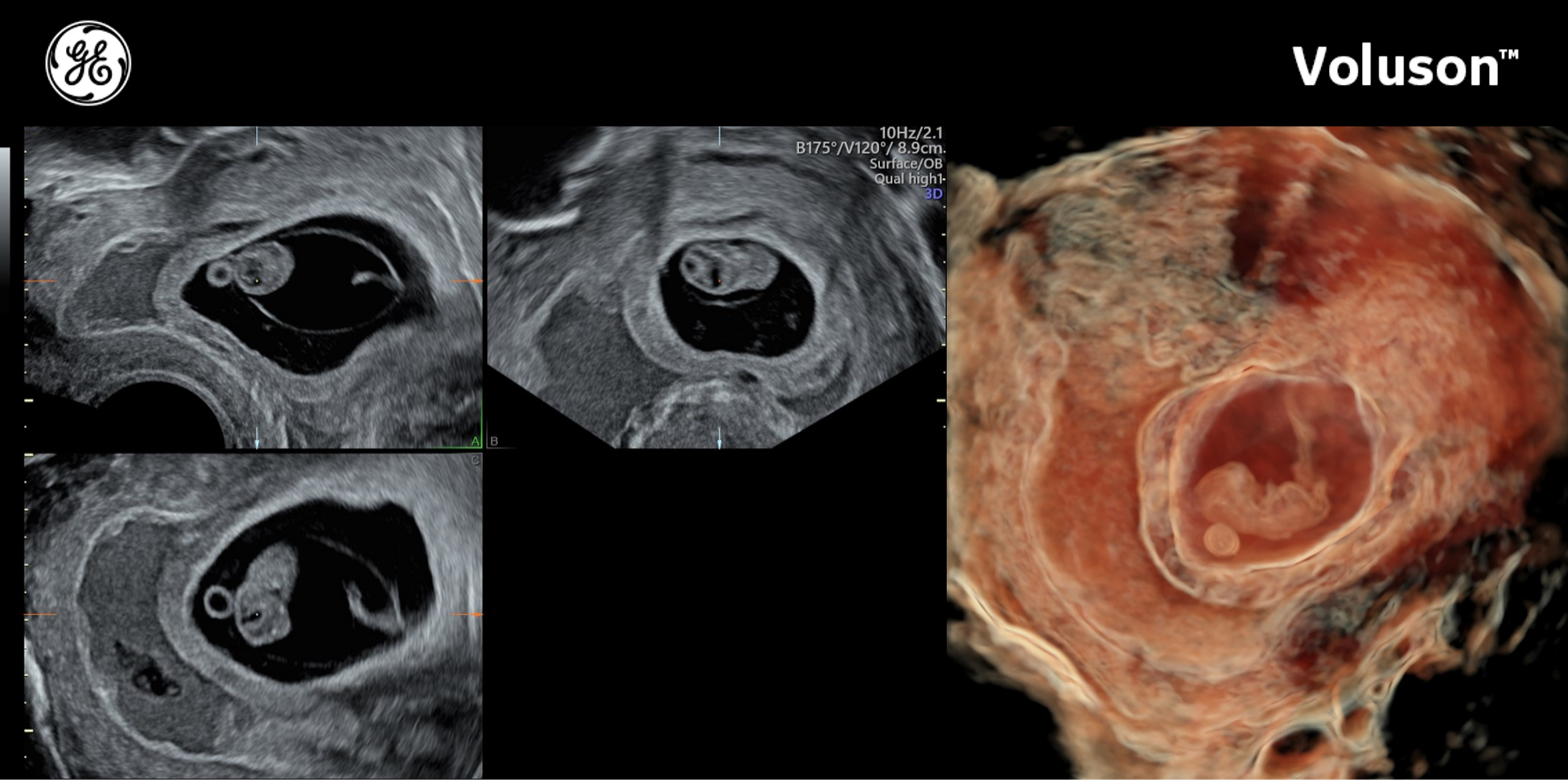
First trimester bleeding caused by a subchorionic hematoma
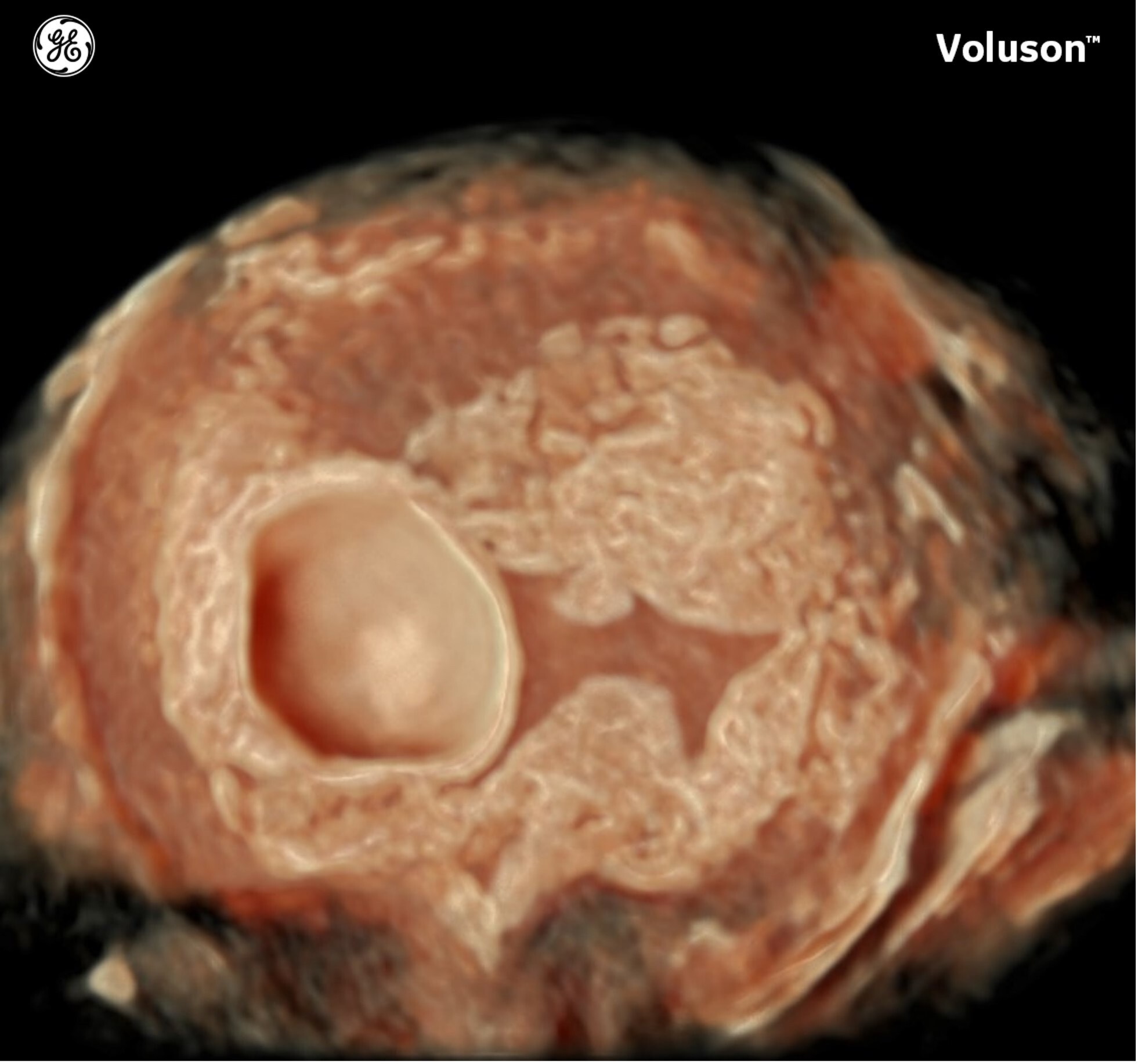
First trimester bleeding caused by a subchorionic hematoma

