While ovarian cysts in teenagers are common, they are still concerning for both patients and clinicians. These fluid-filled structures may be simple or complex and are usually discovered incidentally by physical examination or imaging. Ultrasound imaging plays an important role in differentiating these benign conditions from more serious pathologies.
Prevalence and Potential Complications of Ovarian Cysts in Adolescents
The most frequently diagnosed types of cysts found in adolescent patients are benign, including functional ovarian cysts, dermoid cysts, and cystadenomas. The overall prevalence of ovarian cysts is unknown.
A study in the Journal of Clinical Research in Pediatric Endocrinology showed that 18.8% of girls ages 10 years to 18 years presenting to the pediatric emergency department (ED) with pelvic pain had ovarian cysts.1 Peak ovarian cyst frequency was observed at age 15, with a rate of 31.3%.
Ovarian cysts frequently regress without treatment and are seldom associated with malignancy, but it's important to note that more serious pathologies can also be found in this population. A multicenter study published by the Journal of Pediatric and Adolescent Gynecology showed that most girls have cysts that are considered simple.2 Still, the possibility for coexisting pathologies or complications such as tumors, torsion, and central precocious puberty (CPP) exists.
Additionally, ovarian cysts occasionally cause complications,3 including pelvic pain, cyst rupture, blood loss, and ovarian torsion, all of which necessitate prompt management.
Diagnosing Ovarian Cysts in Teenagers with Ultrasound
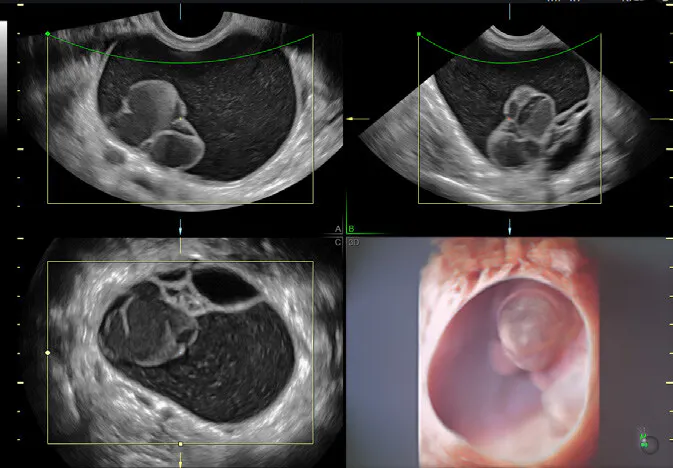
Ultrasound is the preferred diagnostic tool for evaluating ovarian cysts in teenagers. Physicians often turn to ultrasound because of its non-invasive nature, lack of radiation exposure, and efficacy in providing detailed images of the cyst's size, location, and characteristics. Patients appreciate the ease with which clinicians can obtain images with ultrasound and not having to deal with claustrophobia while being imaged.
When diagnosing a cyst on ultrasound, the most crucial question to answer is whether the lesion is benign or malignant. Additionally, for the former, it's important to identify an endometrioma and possible deeply infiltrating endometriosis when making arrangements for surgery.4 For those with malignancies, using ultrasound to predict a mucinous borderline tumor can open the door to fertility-sparing surgery and also identify patients who might need further gastrointestinal assessment.
There are considerable advantages of using transvaginal sonography over conventional transabdominal sonography to diagnose ovarian cysts,5 but transperineal sonography can still be useful when looking at large tumors.
For benign cysts, ultrasound will consistently show thin, smooth walls; an absence of septations; solid components; and internal flow on color Doppler.3 On the other hand, ultrasound findings that indicate the potential for malignancy include a size larger than 10 centimeters, irregularity, high color Doppler flow, papillary or solid components, and the presence of ascites.6
Using Ultrasound to Monitor Patients with Ovarian Cysts
Ultrasound continues to play an important role in the follow-up care of patients with ovarian cysts. These patients are regularly sent for ultrasound monitoring of ovarian cysts, particularly in cases of functional cysts related to the menstrual cycle. Patients with endometriomas should receive follow-up sonograms within six to 12 weeks after initial imaging, then yearly until surgically removed.3 For those with dermoid cysts, yearly follow-up with ultrasound is also advised until surgical removal.
Resources:
- Emeksiz HC, Derinöz O, Akkoyun EB, et al. Age-specific frequencies and characteristics of ovarian cysts in children and adolescents, Journal of Clinical Research in Pediatric Endocrinology, 2017 Mar;9(1): 58–62. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5363166/.
- Aydin BK, Saka N, Bas F, et al. Evaluation and treatment results of ovarian cysts in childhood and adolescence: a multicenter, retrospective study of 100 patients. Journal of Pediatric and Adolescent Gynecology. 2017 Aug;30(4):449–455. https://pubmed.ncbi.nlm.nih.gov/28167139/.
- Mobeen S, Apostol R. Ovarian cyst, StatPearls Publishing, 2024 January. https://www.ncbi.nlm.nih.gov/books/NBK560541/.
- Sayasneh A, Ekechi C, Ferrara L, et al. The characteristic ultrasound features of specific types of ovarian pathology (review), International Journal of Oncology. 2015;46 (2):445–458. https://doi.org/10.3892/ijo.2014.2764.
- Marret H. Doppler ultrasonography in the diagnosis of ovarian cysts: indications, pertinence and diagnostic criteria. Journal de Gynecolologie, Obstetrique et Biologie de la Reproduction. 2001;30 (1):S20–33. https://pubmed.ncbi.nlm.nih.gov/11917373/.
- American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology. Practice bulletin no. 174: evaluation and management of adnexal masses. Obstetrics and Gynecology. 2016 Nov;128(5):e210–e226. https://pubmed.ncbi.nlm.nih.gov/27776072/.