
As evidence mounts in favor of the potential cancer-preventing benefits of bilateral salpingectomy, more patients today are opting for salpingectomy rather than tubal ligation.
Between 2000 and 2013, one study found a 77 percent increase in salpingectomies, while tubal ligation rates decreased. The majority of those increases took place in the latter two years. Similarly, Harvard Medical School reported that in 2008, just 1 in 250 sterilizations was a salpingectomy. Three years later, that ratio surged to 1 in 3.
The trends come in tandem with literature that links salpingectomies to a marked reduction in ovarian cancers. Notably, ovarian cancers that originate in the fallopian tubes are among the most fatal, which makes preemptively removing them an appealing option for certain groups of patients seeking permanent sterilization.
However, fallopian tube removal is not for every patient, and there are other factors to weigh for each sterilization method. Here's what you, and your patients, should know.
Comparing Tubal Ligation and Salpingectomy
Tubal ligation is an effective means of sterilization that has long been considered a standard method for those seeking to permanently prevent pregnancy. In some cases, it can also be reversed. Although tubal ligation does have the potential to reduce the risk of ovarian cancer, its benefits are not nearly as pronounced as those seen with salpingectomy. The removal of the fallopian tubes is also an effective means to prevent pregnancy, but unlike tubal ligation, it cannot be reversed.
In the short term, research published in The Journal of Minimally Invasive Gynecology links bilateral salpingectomy to a slightly longer procedure time if performed postpartum (71 minutes for salpingectomy, compared to 59 minutes for tubal ligation). The procedure time is about equivalent when done during cesarean procedures. It has also shown comparable rates of complications and blood loss when performed both postpartum and during a cesarean.
However, it is the potential long-term protective effects that have triggered such widespread adoption of salpingectomies. For example, a 2015 study published in the Journal of the National Cancer Institute found a significantly lower risk (hazard ratio 0.65) for ovarian cancer in patients who had their tubes removed compared to the general population. A meta-analysis in The Journal of Minimally Invasive Gynecology found that bilateral salpingectomy resulted in a risk reduction between 42 percent and 78 percent, compared to 13 percent to 41 percent with tubal ligation.
Despite the positive findings of cancer protection, some physicians still exercise caution before opting for total tube removal, especially among low-risk patients or those who are not otherwise undergoing pelvic surgery for benign reasons.
Because salpingectomy could trigger early menopause, it may lead to various negative consequences of hormone reduction, such as heart disease. For patients without a family history of breast or ovarian cancer or other risk factors, the decreased cancer risks may not be enough to offset these other long-term health risks.
Ultrasound a Vital Tubal Tool for Tubal Evaluation
Whichever method is best for your patients, ultrasound can be a vital tool for tubal evaluation both before and after sterilization. In tubal ligation, for example, ultrasound can help confirm the procedure successfully blocked the tubes by checking for fluid movement or by evaluating for ectopic pregnancy, which is a risk with tubal ligation. In salpingectomy, researchers continue to use ultrasound to monitor follicle size and blood flow to oversee hormonal changes that could potentially prompt greater health risks.
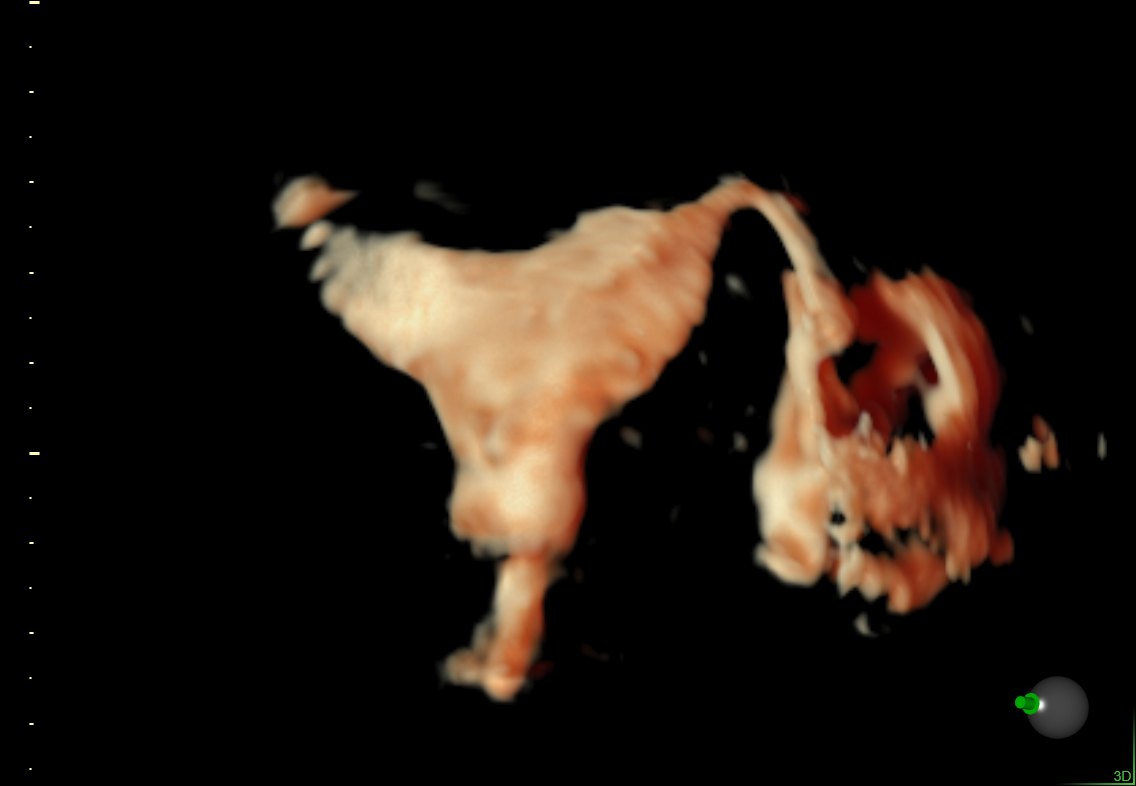
HyCoSy demonstrating patent left fallopian tube.
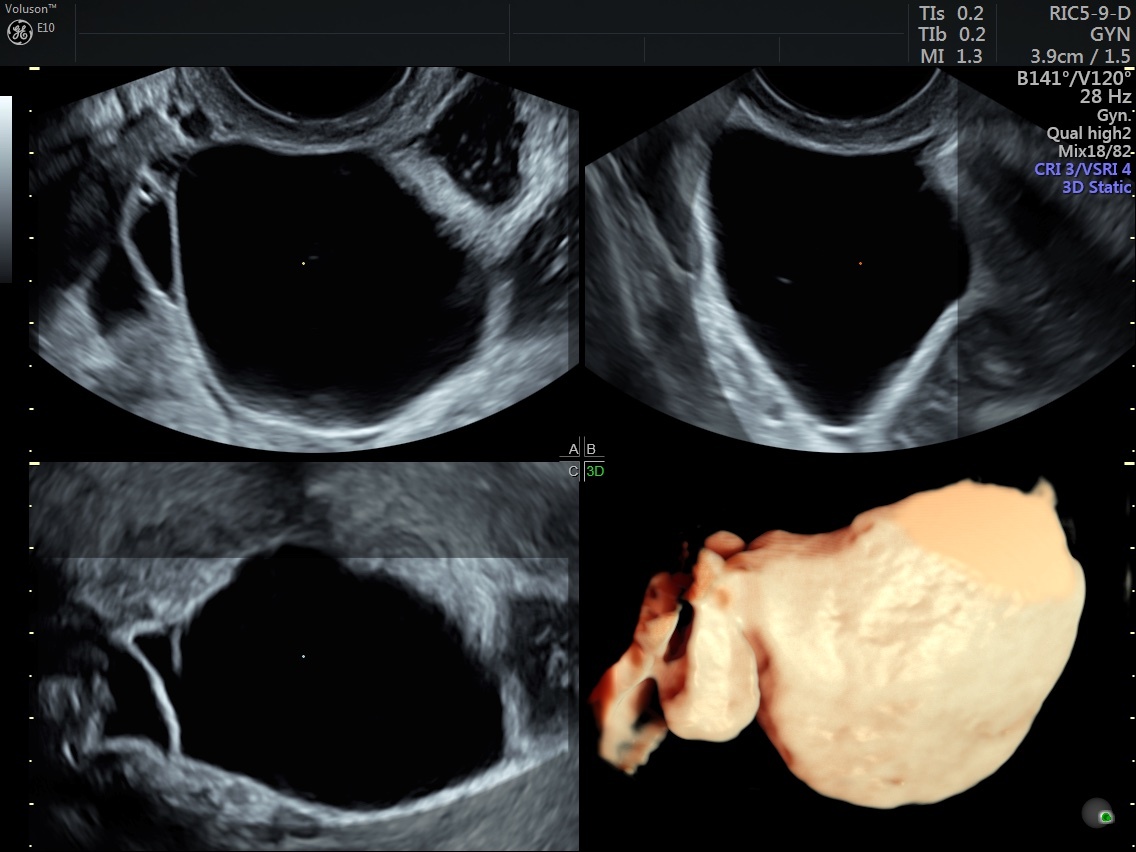
3D ultrasound hydrosalpinx.

