In today's healthcare landscape, the significance of accurate ultrasound diagnosis cannot be overstated. The correct identification of female reproductive healthcare conditions is the key to providing timely optimal treatment methods, which will notably impact patient outcomes. The need for accurate diagnosis is particularly crucial in cases of adenomyosis. This condition occurs when endometrial tissue grows within the uterine walls and is associated with serious complications that can affect women's health and fertility.
The Importance of Correct Diagnosis of Adenomyosis
Accurate diagnosis forms the bedrock of effective treatment. When dealing with adenomyosis, a precise understanding of the condition enables healthcare providers to select the most appropriate treatment tailored to the patient's needs. Accurate diagnosis can help prevent unnecessary surgeries and risky exploratory procedures. It also minimizes incorrect treatments that might exacerbate the condition, cause complications, or lead to unnecessary patient suffering.
Furthermore, correct diagnosis plays a crucial role in identifying high-risk obstetrical patients. Adenomyosis has been linked to several obstetric risks, including preeclampsia, preterm labor, intrauterine growth restriction (IUGR), placenta previa, and stillbirth. Early detection through accurate diagnosis empowers healthcare providers to deliver proactive care and mitigate potential risks during pregnancy.
Complications Associated with Adenomyosis
Adenomyosis is a complex disease that can coexist with other uterine abnormalities and cause numerous complications. Studies indicate a correlation between this condition and infertility, anaemia, and increased miscarriage rates among affected women. Moreover, adenomyosis is significantly associated with various obstetric risks, including preeclampsia, preterm labor, small fetal size for gestational age, IUGR, and stillbirth. The serious complications of adenomyosis highlight the need for early detection and management.
Diagnostic Tools and Advancements
Contrary to some misconceptions, advanced diagnostic tools like MRI and transvaginal ultrasound offer detailed and reliable assessments of the female pelvis for adenomyosis. These two diagnostic methods have comparable quality and accuracy. Notably, ultrasound diagnosis of adenomyosis is both cost-effective and widely accessible. This tool reduces waiting times and facilitates early detection, providing the most efficient means for identifying and diagnosing adenomyosis.
Identifying Adenomyosis Through Ultrasound
Understanding the various adenomyosis signs and symptoms is crucial for identifying this disease. Clinicians can use transvaginal ultrasound to identify direct or indirect signs of adenomyosis. These key indicators can guide healthcare providers to an accurate diagnosis.
Uterine Shape
Adenomyosis can be subtle, but its presence changes the overall shape of the uterus. Muscular hypertrophy of the uterine myometrium causes it to appear more round and globular. Complications of this sign can include the presence of small fibroids and deep infiltrative endometriosis (which can cause caudal distortion of the uterus). The patient's use of oral contraceptives (which can make the uterus appear more round) can also contribute to the difficulty of this diagnosis.
Asymmetric Uterine Walls
Adenomyosis tends to affect one side of the uterus more than the other. Clinicians should assess the uterus carefully and compare the anterior myometrial wall with the posterior, or the left myometrial wall with the right. Noticeable thickness of one side of the uterus over the opposite is a direct indication of adenomyosis. Taking a uterine wall thickness measurement when assessing for adenomyosis is a crucial step in identifying this sign. The presence of a uterine contraction, which is most often seen when ovulation is near, can be a hindrance.
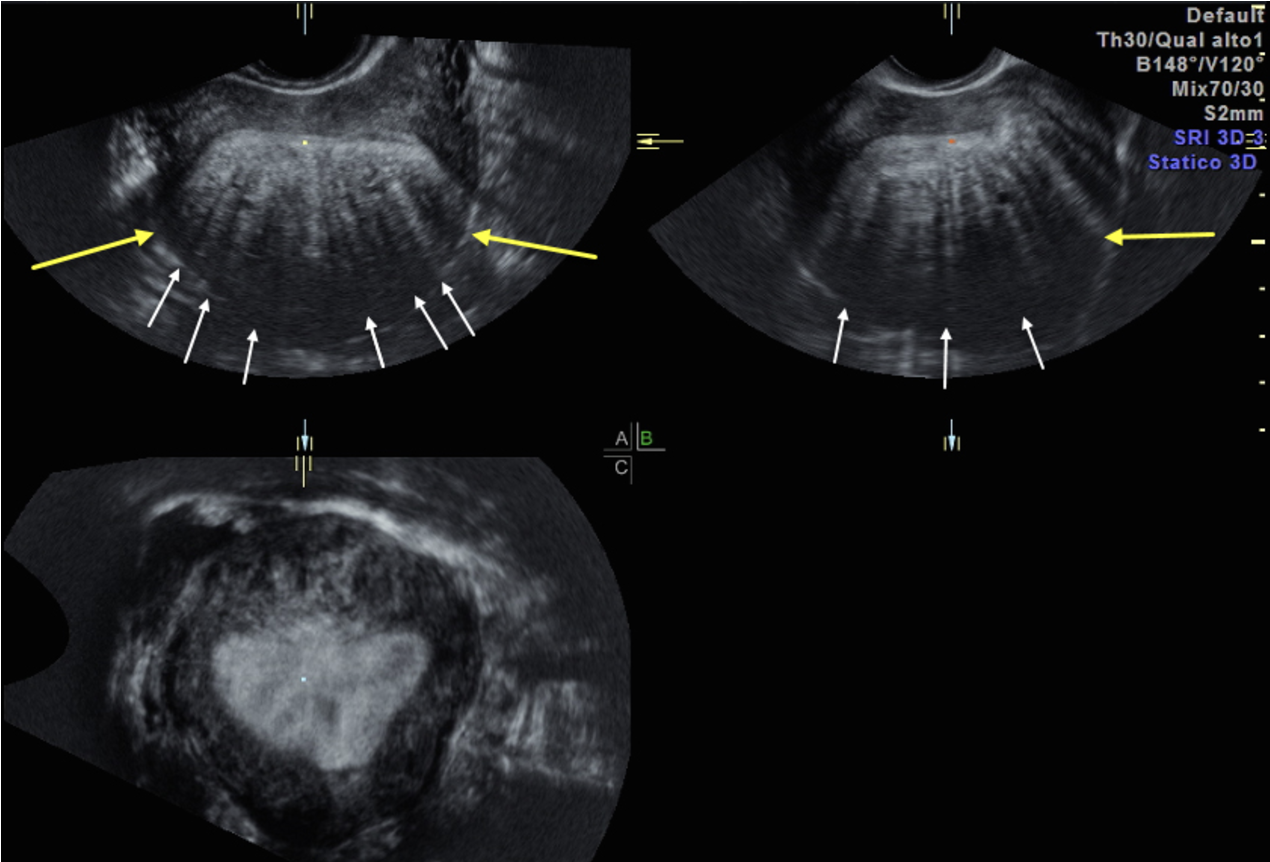
Adenomyosis showing asymmetric uterus (yellow arrows) and linear shadowing (white arrows)
Fan-Shaped Echogenicity
When sweeping through the uterus, you will notice areas of brighter posterior enhancement in a very clear fan-shape that's narrower at the top and wider at the bottom. Echogenicity can also appear as stripes of brighter enhancement with darker shadowing. This pattern is caused by circular layers of hypertrophic muscle fibers that surround the foci of adenomyosis within the myometrium. The pitfalls of this indirect sign can include the stripes of posterior shadowing seen with fibroids, in which case the focal mass of the fibroid must be identified. Another obstacle is the presence of uterine vessels within and around the uterus, which can sometimes cause a striped shadow and enhancement appearance. Clinicians can use power Doppler imaging to identify the presence of vessels.
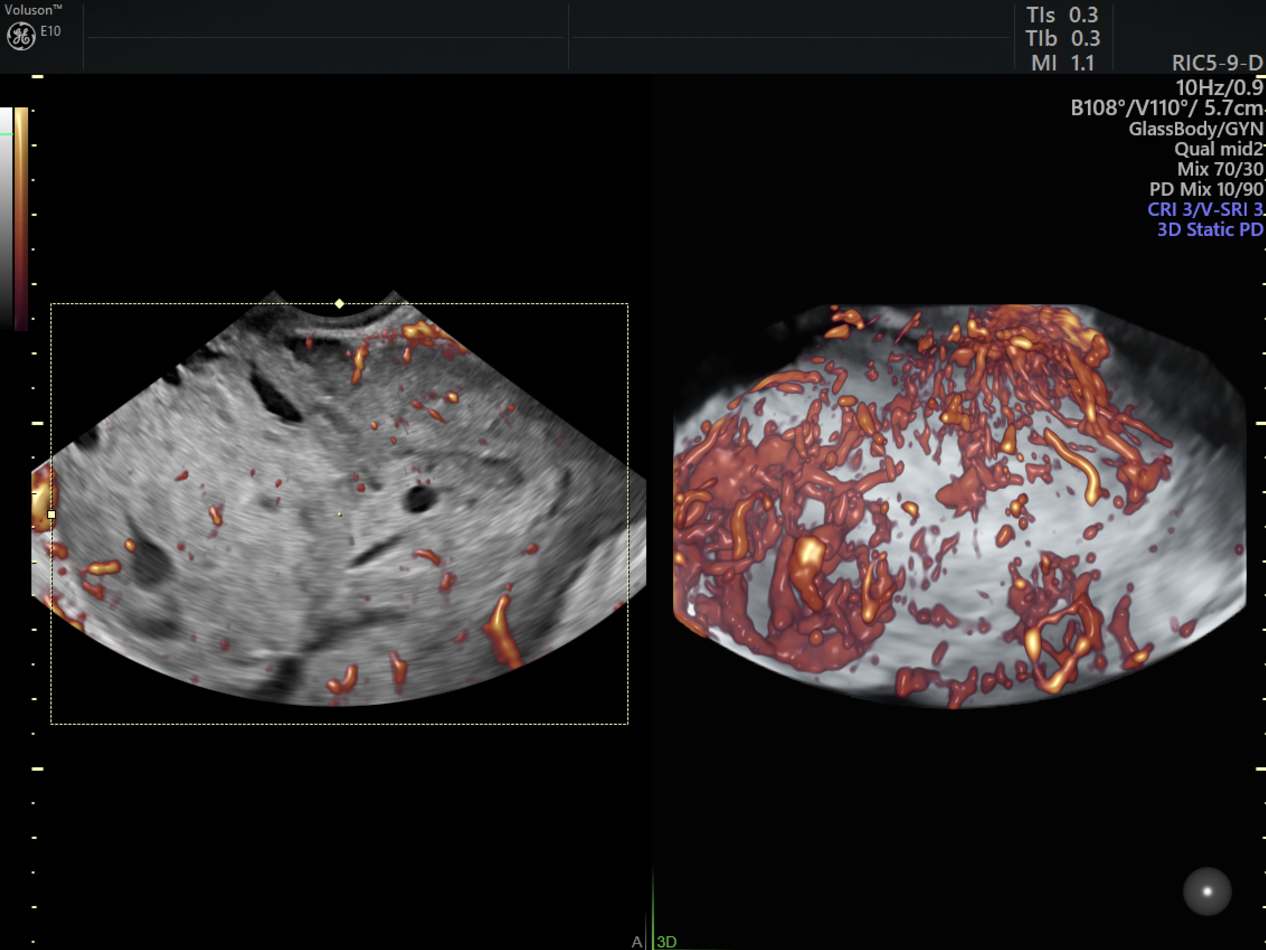
Adenomyosis vascular pattern shows blood flow through the area, in a non-circular pattern
Myometrial Alteration
These findings include direct markers, such as the appearance of hyperechoic islands or islets, which are focal echogenic areas within the myometrium. Other indicators include myometrial cysts, which appear anechoic, and/or shadows within the myometrium, which appear hypoechoic. Difficulties of these signs can also be caused by the presence of uterine vessels within and around the myometrium. Power Doppler imaging, with its increased sensitivity to low flow, is crucial for determining if the echogenic areas are from adenomyosis (no color Doppler) or vessels (will contain color Doppler). Additionally, identifying an echogenic rim around a myometrial cyst will demonstrate the presence of ectopic endometrium within the myometrium, which is a clear signal of adenomyosis.
Irregular Junctional Zone
This sign is caused by direct invasion of adenomyosis from the endometrium into the myometrium and presents as a poorly defined or irregular border around the endometrium. The use of 3D ultrasound with the coronal view is highly effective in identifying this direct indicator of adenomyosis. Obstacles to this marker can occur with operator variability, as this finding is highly dependent on the examiner. Focusing attention on identifying a normal junctional zone can be more effective during ultrasound assessment. The presence of a normal junctional zone will exclude adenomyosis with a high certainty from that case if no other signs are identified, or if others are non-specific.
Differentiating Adenomyoma from Fibroids
It's crucial to distinguish an adenomyoma—or the nodular aggregate of endometrial glands within the myometrium—from a fibroid. On ultrasound, an adenomyoma appears as a subtle hypoechoic area with ill-defined borders (no capsule) and diffuse, trans lesional vascularization (with power Doppler). By contrast, a fibroid has a capsule and a clearly defined border with circular peripheral vascularization. It's important to be able to differentiate between these conditions for treatment purposes.
When a fibroid is present in the uterus, it displaces and pushes aside the normal myometrial tissue. Consequently, healthy and strong muscle remains in that area of the uterus even after surgical fibroid removal. Fibroids leave the myometrial integrity intact, making it possible to have safe future pregnancies. In contrast, the presence of adenomyosis in the uterus destroys the myometrial tissue. Thus, if an adenomyoma is present, there may not be enough healthy myometrial tissue remaining after removal to close a wound in that area, resulting in impaired myometrial integrity. Patients with impaired myometrial integrity are at risk of uterine rupture if they become pregnant. Therefore, a definitive distinction between fibroids and adenomyosis is crucial for appropriate treatment planning considering the impact on myometrial integrity and the associated risks for future pregnancies.
It's evident that the relevance of accurate ultrasound diagnosis in identifying adenomyosis is imperative. Early detection through reliable diagnostic tools like ultrasound empowers healthcare providers to deliver tailored treatments, mitigate obstetric risks, and offer the best care for affected patients.
Watch Dr. Tellum's video HERE.