
Enhanced myometrial vascularity (EMV) may be an unfamiliar term for patients and healthcare providers alike. Although physicians and researchers previously used the term uterine arteriovenous malformations (AVMs), recent research has shown that this older terminology can hinder effective diagnosis and care.
In most cases, pathology identified as intense uterine vascularity via color Doppler is not true uterine arteriovenous malformation. Instead, the real foci of intense uterine vascularity are often enhanced myometrial vascularity, which has a different pathogenesis from congenital arteriovenous malformations.
EMV and RPOC
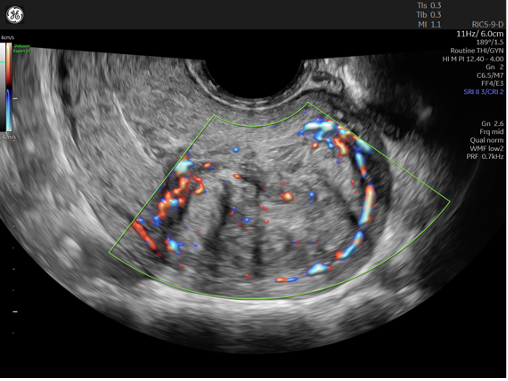
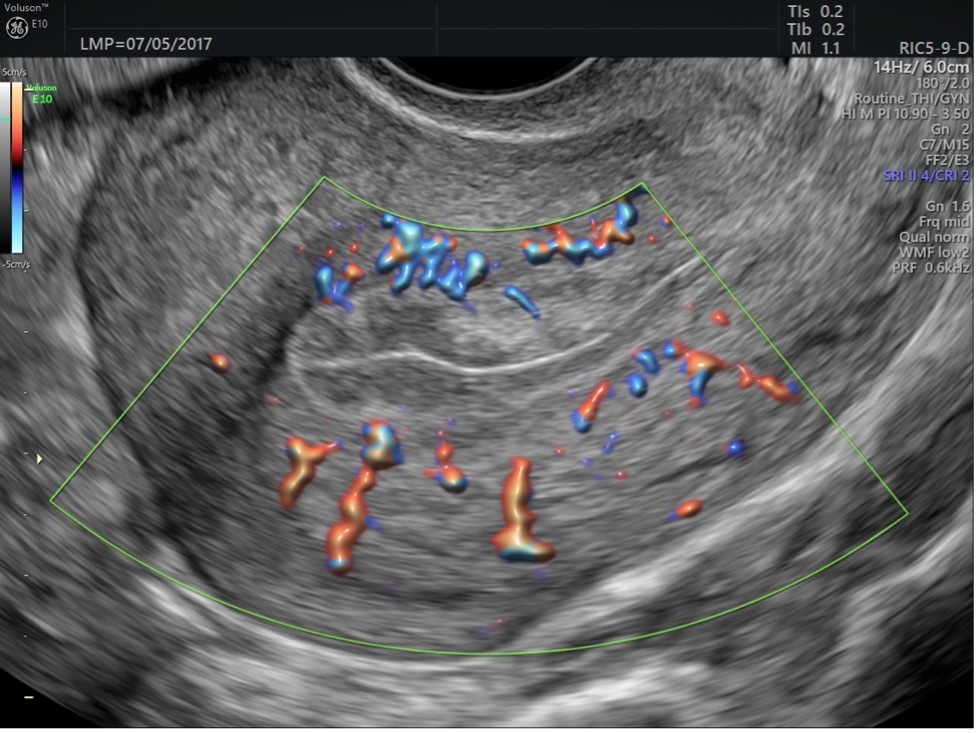
Most occurrences of these intense vascularity bundles, now commonly known as EMV, are associated with early pregnancy loss and retained products of conception (RPOC), according to research published in Ultrasound in Obstetrics and Gynecology. Retained placenta following a vaginal delivery or cesarean section may also yield the state of EMV. In most of the cases where EMV is identified, transvaginal pelvic ultrasound has been used to evaluate for uterine bleeding abnormalities after pregnancy.
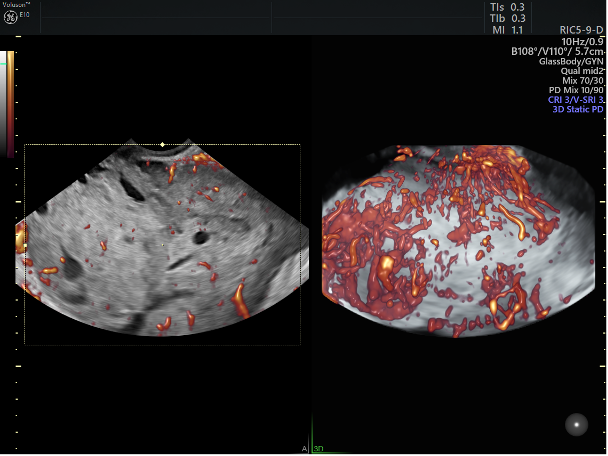
Color Doppler is the key sonographic tool for the identification of EMV, though RPOC are generally visible on 2D ultrasound. 3D ultrasound is useful for evaluating intracavitary pathology — in this case, RPOC — but will not likely aid in the diagnosis of EMV.
Safe, Effective Surgical Treatment for RPOC and EMV
When RPOC is identified and has associated EMV, medical or surgical procedures to resolve the retained tissue are generally safe and do not result in severe, life-threatening bleeding, according to separate research published by Ultrasound in Obstetrics and Gynecology. The historic and incorrect label of arteriovenous malformation in a post-pregnancy state implied there would be a serious and likely life- or uterus-threatening bleeding event if surgical management in the form of dilatation and curettage (D&C) were implemented.
A paper published in the Journal of Obstetrics and Gynaecology explains that this misunderstanding caused unnecessary concern among many OB/GYNs, resulting in either overtreatment with interventional procedures to embolize the arteriovenous malformations or undertreatment, forgoing D&Cs that may have helped resolve patients' postpregnancy bleeding abnormalities.
A postpregnancy state, especially following pregnancy loss, is often a time of extreme stress for patients. When the course of care goes awry with retained tissue and abnormal bleeding, a positive result hinges on optimal and timely resolution of the problem. Incorrectly classifying patients as having an arteriovenous malformation yields an extra layer of emotional and even physical strain on the patient and their family.
EMV and Other Uterine Pathology
While abnormal uterine bleeding postpregnancy is a clear indication to evaluate for retained tissue and EMV, physicians must be aware of other uterine pathology. It is important to note that congenital arteriovenous malformations are extremely rare; the literature includes fewer than 100 published case reports. These malformations are not likely to present in a post-pregnancy state where retained tissue is identified.
Beyond understanding the clinical presentations, providers should use ultrasound features to differentiate between EMV and other pathology. Overall, OB/GYNs can lean on guidance from the Morphologic Uterine Sonographic Assessment (MUSA) and the International Endometrial Tumor Analysis groups.
Fibroids and adenomyosis are two common myometrial issues, and each has unique features. Fibroids can be variable in appearance, but they generally appear as spherical structures with circumferential vascular patterns on color Doppler.
Fibroid shown using color Doppler
Adenomyosis also varies in appearance, arguably more so than fibroids. Some cases present translesional vascularity, which represents an indirect feature of adenomyosis. Although the descriptor suggests vascularity that traverses a "lesion" (i.e., an adenomyoma), the latest MUSA update suggests this vascular pattern does not necessarily have to traverse an obvious adenomyoma; it can simply be present in the context of other adenomyosis features.
Adenomyosis shown using color Doppler
Differential Diagnosis: Endometrial Polyps
Clinicians may also have to consider intracavitary pathology such as endometrial polyps and endometrial hyperplasia or malignancy. In some ways, endometrial polyps share features of abnormal uterine bleeding with retained tissue and EMV. Polyps can lead to erratic spotting, although they are not generally problematic immediately after a pregnancy state. They may appear more regular than retained tissue, and they will generally be minimally, if at all, vascular. The classic vascular pattern for a polyp on color Doppler is a single feeding vessel.
Uterine polyp shown with color Doppler
Cancer and precancerous states, however, may have more ample blood flow; this is usually a concerning feature for more advanced stages of the disease. Although endometrial cancer may share most in common with RPOC/EMV from an ultrasound perspective — a thickened and irregular endometrial lining with adjacent myometrial vascularity — the population is dramatically different, and the clinical picture is usually evident (namely postmenopausal bleeding versus post-pregnancy abnormal uterine bleeding).
Planning EMV Treatment
A solid understanding of a patient's clinical history, supported by ultrasound images obtained and interpreted by someone with a strong awareness of EMV, can be enough to get the patient on the right treatment path.
Even when these vascular foci are mislabelled as post-pregnancy arteriovenous malformations, clinicians can be reassured that they are not actually arteriovenous malformations — nor are they dangerous. Oftentimes, it is more dangerous, both physically and emotionally, to subject patients to procedures meant to treat an arteriovenous malformation; or, conversely, to let them continue to bleed with retained pregnancy tissue out of fear that a medical or surgical procedure will cause serious harm. Unlike true arteriovenous malformations, retained tissue is common. Mounting evidence suggests associated EMV may be as well.
Prompt and accurate diagnosis of EMV is essential to effectively treating patients; ultrasound is a powerful tool that can help OB/GYNs and other clinicians decipher the patient's concerns with a high degree of accuracy. As the technology continues to advance, ultrasound can help clinicians differentiate between most endometrial-myometrial pathologies and identify enhanced myometrial vascularity associated with retained pregnancy tissue.

