

Like most great pretenders, ovarian torsion mimics other, more common medical emergencies, such as ruptured ovarian cysts, ectopic pregnancy and even appendicitis. A relatively rare condition, it has been detected in women of all ages and even a fetus, according to a study published in Ultrasound in Obstetrics & Gynecology and presented at the 26th World Congress on Ultrasound in Obstetrics and Gynecology. The astute physician will recall that the differential diagnosis includes ovarian torsion and will then clinch the diagnosis through an ovarian torsion ultrasound evaluating the pelvis.
Sudden in onset, the pain associated with ovarian torsion can be severe and worsen with activity. It is usually unilateral and sometimes associated with nausea, vomiting, low-grade fever and mild leukocytosis. No age group is spared. With ovarian torsion, the right ovary is frequently involved, but, on occasion, it is bilateral. It can occur in pregnancy, and a delay in diagnosis is not uncommon.
Using Ultrasound To Evaluate Signs of Ovarian Torsion
Ovarian torsion can be intermittent, partial or complete. It may also involve the fallopian tube, in which case it is termed an adnexal torsion. As a result of the twisting of the ovary around its ligamentous support, the blood supply to and from the ovary may be compromised.
Ovarian torsion ultrasound findings may vary, but a unilateral enlarged (>4 cm) edematous ovary with peripheral cysts and free pelvic fluid is pathognomonic. The peripherally displaced follicles are due to the engorged central ovarian parenchyma. Often a coexisting ovarian mass may be present, because cysts and tumors can increase the size and weight of the ovary, predisposing it to torsion.
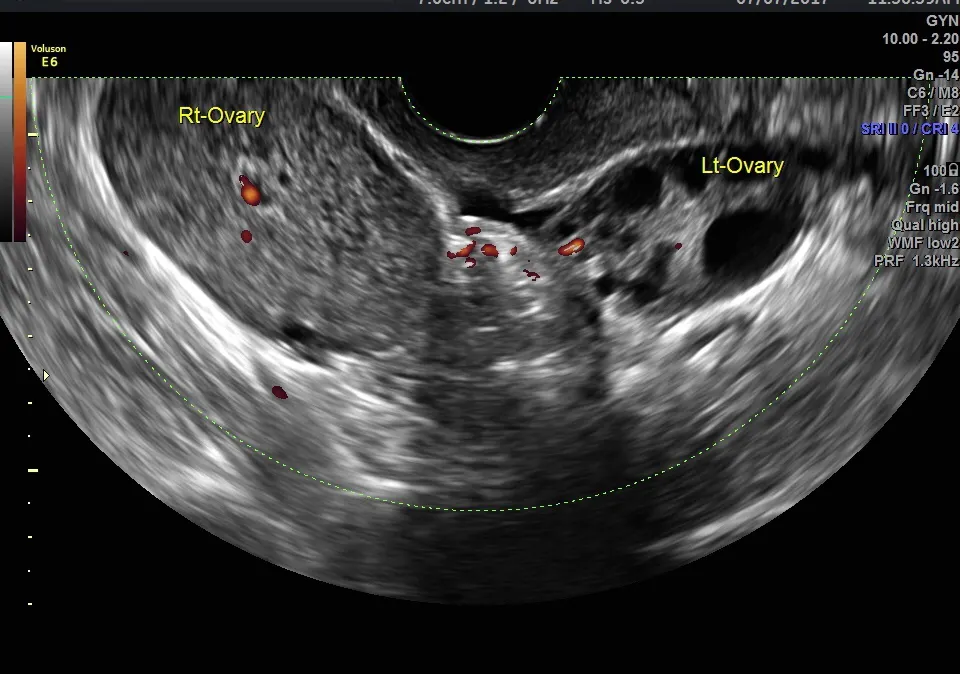
Avoid assuming this mass is the cause of the patient's pain. Use a Doppler ultrasound to determine whether there is blood flow to the ovary. The classic whirlpool sign of the ovarian vascular pedicle may be present. Venous blood flow disappears first, then arterial. If there is evidence of blood flow, especially if blood flow is present in the interior of the ovary, it does not exclude torsion but may suggest that a viable ovary exists.

Ovarian torsion ultrasound image one

ovarian torsion ultrasound image two
ovarian torsion ultrasound image three
Treating Ovarian Torsion
If not attended to urgently, the ovary may be unsalvageable and require removal. Unfortunately, the severity of the symptoms does not predict the viability of the ovary. Hence, mild ovarian torsion symptoms can be associated with a nonviable ovary. Ovarian torsion is prevalent in adolescents, so proper diagnosis and treatment is imperative to ensure that there is no compromise to future fertility.
Simple untwisting of the ovary, with or without oophoropexy or ovarian ligament plication (in the case of an unusually long ligament), is recommended in the juvenile female and women wishing to optimize fertility. Caution is warranted regarding even simple cystectomy and biopsy because any assault on the ovary may reduce ovarian reserve. If an ovarian malignancy is suspected, appropriate surgical staging is indicated with proper preoperative surgical consent.
The diagnosis of ovarian torsion can be a challenge. A high degree of clinical suspicion, coupled with rapid evaluation, will serve the clinician and patient well. Ultrasound, combined with Doppler assessment of blood flow to the affected ovary, is your best diagnostic tool when a patient presents with acute onset unilateral pelvic pain.



